School Refusal in Autistic Children: The Iceberg Model and What Actually Helps
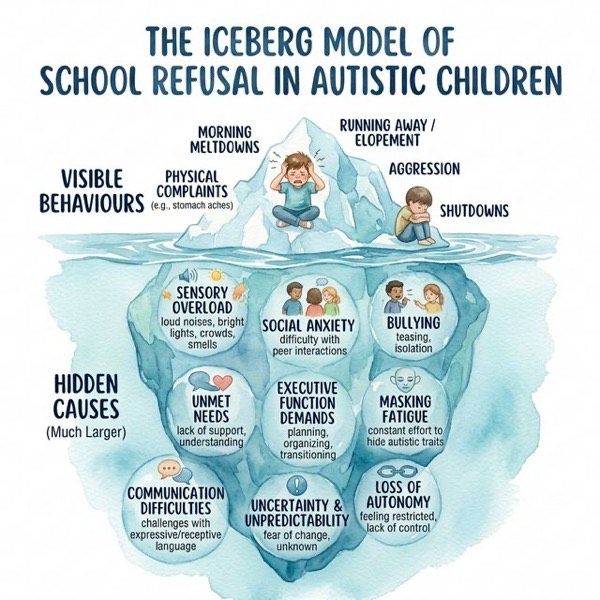
When an autistic child stops going to school, the visible behaviours, such as morning meltdowns, physical complaints, running away, aggression, or complete shutdown, are only the tip of the iceberg. Beneath the surface lies a much larger mass of hidden causes that, if left unaddressed, will ensure that no amount of reward charts, attendance targets, or pressure will get that child back through the school gates.
This article uses the iceberg model to explain what drives school refusal in autistic children, what the evidence tells us about effective approaches, and what parents and professionals can do.
The Iceberg Model
The iceberg model is a widely used framework in autism practice. It recognises that the behaviours we can see (above the waterline) are driven by factors we often cannot see (below the waterline). In school refusal, this distinction is critical, because interventions that target only the visible behaviour, such as attendance penalties or rewards for going to school, will fail if the underlying causes remain.
Above the Waterline: What You See
These are the behaviours that trigger referrals, attendance meetings, and parental distress:
- Morning meltdowns: Extreme distress on school mornings, often escalating as the departure time approaches
- Physical complaints: Headaches, stomach aches, nausea, and vomiting that are genuine physiological stress responses, not fabrication
- Running away or elopement: Leaving the classroom, hiding in school, or running from the school building
- Aggression: Directed at parents, siblings, or school staff, often during attempts to force school attendance
- Complete shutdown: The child becomes mute, immobile, or dissociative — the opposite of a meltdown but equally distressing
Below the Waterline: What You Cannot See
These are the drivers. Each child’s iceberg will look different, but research consistently identifies the following factors:
Sensory Overload
School environments are a sensory assault for many autistic children. Fluorescent lighting, echoing corridors, the smell of school dinners, crowded playgrounds, hand dryers in toilets, unexpected fire alarms, and the constant background noise of 30 children in a classroom. Research shows that sensory processing differences are present in over 90% of autistic individuals, and that sensory overload is a significant predictor of anxiety and school avoidance (1).
Social Anxiety and Social Demands
Unstructured social time, particularly break and lunchtime, is consistently reported as the most stressful part of the school day. Navigating peer relationships, understanding unwritten social rules, and the constant effort of social interaction can be exhausting. Many autistic children describe playtime as the worst part of school (2).
Bullying
Autistic children are significantly more likely to be bullied than their neurotypical peers. A meta-analysis found that 44% of autistic children experience bullying, compared to approximately 10-15% of the general school population. Bullying may be overt (name-calling, physical aggression) or covert (social exclusion, manipulation), and autistic children may struggle to identify or report it (3).
Executive Function Demands
Schools demand constant executive functioning: organising equipment, transitioning between activities, managing time, following multi-step instructions, coping with changes to routine, and switching between tasks. For children whose executive function is already challenged, the cumulative cognitive load can become overwhelming (4).
Masking Fatigue
Many autistic children, particularly girls and those without intellectual disability, learn to “mask” their autistic traits at school, suppressing stimming, imitating peers’ social behaviour, and hiding their distress. This requires enormous cognitive and emotional effort. Research by Cage and Troxell-Whitman found that masking is associated with increased anxiety, depression, and autistic burnout. The child may appear to cope at school but collapse at home (5).
Unmet Needs and Inadequate Support
When a child’s EHCP (Education, Health and Care Plan) is not implemented, when teaching assistants are reassigned, when reasonable adjustments are not made, or when staff do not understand autism, the child’s needs go unmet. The gap between what a child needs and what they receive creates chronic stress.
Communication Difficulties
The inability to articulate what is wrong, to ask for help, or to explain their experience means that distress accumulates without release. Verbal children may still lack the emotional vocabulary to explain their internal state.
Uncertainty and Unpredictability
Supply teachers, timetable changes, cancelled activities, classroom rearrangements, and the general unpredictability of a typical school day can create constant anxiety for children who rely on predictability and routine.
Loss of Autonomy
Schools require children to comply with adult-directed activity for hours at a time, with limited choice over what they do, when they do it, whom they sit with, and when they eat, drink, or use the toilet. For some autistic children, this loss of control is a significant source of distress.
Prevalence and Terminology
School refusal in autistic children is extremely common. A survey by the National Autistic Society found that 33% of autistic children had been formally or informally excluded from school, and a further significant proportion had reduced timetables or were on part-time attendance. The term “school refusal” itself is contested; many families and professionals prefer “school avoidance” or “Emotionally Based School Avoidance” (EBSA) to reflect that the child is not choosing to refuse but is unable to attend due to overwhelming distress (6).
The EBSA framework, now adopted by many local authorities in England, explicitly recognises that non-attendance is a symptom rather than a problem to be solved through enforcement.
What the Evidence Says About What Helps
1. Identify and Address the Underwater Factors
The single most important step is to stop focusing on attendance and start investigating what is driving the avoidance. This requires:
- A thorough assessment of the child’s sensory profile and the school’s sensory environment
- A review of social experiences, including specific questioning about bullying
- Assessment of the child’s mental health (anxiety, depression, trauma)
- Review of the EHCP or support plan and whether it is being implemented
- Talking to the child (if they can communicate their experience) about what specific aspects of school are difficult
2. Reduce Demands Before Increasing Them
Trying to force an anxious child back to full-time attendance quickly is likely to increase distress and entrench avoidance. Evidence supports a graded, flexible approach:
- Start with whatever the child can manage, even if that is 30 minutes in a quiet room
- Build up very gradually, at the child’s pace
- Provide a safe space in school that the child can access when overwhelmed
- Allow flexible start and end times
- Consider reduced timetables as a temporary measure (but with a plan for gradual increase) (7)
3. Modify the Environment, Not Just the Child
Reasonable adjustments that can make a significant difference include:
- Sensory modifications: Ear defenders, sunglasses, seated away from fluorescent lights, permission to leave before the bell for transitions, alternative dining arrangements
- Structured social support: Facilitated social groups, a named safe person, structured lunchtime activities
- Predictability: Visual timetables, advance warning of changes, consistent staffing
- Communication support: Visual supports, a “feelings thermometer,” access to a trusted adult
- Reduced demand: Shorter days initially, choice of tasks, modified homework expectations
- Safe space: A quiet, low-stimulus area the child can access without having to ask permission (8)
4. Therapeutic Support
Cognitive behavioural therapy (CBT) adapted for autistic children has the strongest evidence base for anxiety-driven school avoidance. Key adaptations include:
- Visual and concrete approaches rather than abstract discussion
- Longer treatment duration (autistic children typically need more sessions)
- Incorporation of special interests as motivators
- Explicit teaching of emotional recognition and regulation
- Parent involvement in sessions
Other approaches with emerging evidence include:
- ACT (Acceptance and Commitment Therapy) for adolescents
- Collaborative and Proactive Solutions (Greene’s approach), which focuses on identifying lagging skills and unsolved problems
- Art therapy and play therapy for younger children (9)
5. Collaborative Working
The most effective interventions involve genuine collaboration between parents, school, and external professionals. This means:
- Listening to parents, who know their child best
- Shared planning with clear roles and responsibilities
- Regular review and adjustment of plans
- Consistency between home and school approaches
- Avoiding blame (of the child, the parents, or the school)
6. Consider Whether the Placement Is Right
This is the question nobody wants to ask, but sometimes the answer is that the current school placement is not meeting the child’s needs and cannot be modified sufficiently to do so. In these cases, options include:
- Transfer to a different mainstream school with a different ethos or better resources
- Specialist resource base or additionally resourced provision within mainstream
- Special school placement
- Alternative provision
- Home education (elective home education or local authority-funded home tuition)
Research by Brede et al. found that for many autistic children who had been out of school, a change of placement — particularly to a smaller, more autism-aware setting — was the most significant factor in successful re-engagement (10).
What Not to Do
The evidence is equally clear about what does not work and what causes harm:
- Attendance penalties and fines: Fining families of autistic children for non-attendance penalises disability. It increases parental stress without addressing the cause. Several local authorities have been successfully challenged on this practice.
- Forced attendance: Physically forcing, carrying, or coercing a child into school causes trauma and deepens avoidance.
- Withdrawal of support as punishment: Removing a child’s school place, reducing their EHCP provision, or threatening alternative provision as a consequence of non-attendance is both harmful and potentially unlawful.
- Blaming the parents: Suggesting that the child would attend if the parents were firmer, or framing the problem as a parenting issue, ignores the evidence and damages the collaborative relationship needed for recovery.
- Waiting for the child to grow out of it: Untreated school avoidance tends to worsen, not improve (11).
The Long View
Recovery from school refusal is typically slow. Research suggests that for autistic children, re-engagement with education takes months to years, not weeks. Families need to be supported through this process with realistic expectations, ongoing professional input, and flexibility from educational settings.
The goal should not simply be “get the child back to school.” It should be “help the child access education in a way that does not cause them harm.” For some children, that will be mainstream school with adjustments. For others, it will be specialist provision. For some, it will be a period of home education while therapeutic work takes place.
What matters is that the child’s wellbeing is prioritised, that the underwater causes are addressed, and that the adults around the child work together rather than against each other.
A Note for Parents
If you are reading this because your child is refusing school, know this: you are not failing as a parent. Your child is not being naughty. The research consistently shows that school refusal in autistic children is driven by genuine distress and that the most important thing you can do is listen to your child, advocate for appropriate support, and resist pressure to force attendance when your child is telling you (with their behaviour, if not their words) that they cannot cope.
You know your child. Trust that knowledge.
References
- Green SA, Ben-Sasson A, Soto TW, Carter AS. Anxiety and sensory over-responsivity in toddlers with autism spectrum disorders: bidirectional effects across time. Journal of Autism and Developmental Disorders. 2012;42(6):1112-1119.
- Humphrey N, Lewis S. “Make me normal”: The views and experiences of pupils on the autistic spectrum in mainstream secondary schools. Autism. 2008;12(1):23-46.
- Maïano C, Normand CL, Salvas MC, Moullec G, Aimé A. Prevalence of school bullying among youth with autism spectrum disorders: A systematic review and meta‐analysis. Autism Research. 2016;9(6):601-615.
- Kenworthy L, Yerys BE, Anthony LG, Wallace GL. Understanding executive control in autism spectrum disorders in the lab and in the real world. Neuropsychology Review. 2008;18(4):320-338.
- Cage E, Troxell-Whitman Z. Understanding the reasons, contexts and costs of camouflaging for autistic adults. Journal of Autism and Developmental Disorders. 2019;49(5):1899-1911.
- National Autistic Society. School Report. 2021. Available at: https://www.autism.org.uk/what-we-do/campaign/school-report
- Thambirajah MS, Grandison KJ, De-Hayes L. Understanding School Refusal: A Handbook for Professionals in Education, Health and Social Care. London: Jessica Kingsley Publishers; 2008.
- Autism Education Trust. Schools Guide: Autism and Education. 2019. Available at: https://www.autismeducationtrust.org.uk/
- Chalfant AM, Rapee R, Carroll L. Treating anxiety disorders in children with high functioning autism spectrum disorders: A controlled trial. Journal of Autism and Developmental Disorders. 2007;37(10):1842-1857.
- Brede J, Remington A, Kenny L, Warren K, Pellicano E. Excluded from school: Autistic students’ experiences of school exclusion and subsequent re-integration into school. Autism & Developmental Language Impairments. 2017;2:1-20.
- Munkhaugen EK, Gjevik E, Pripp AH, Sponheim E, Diseth TH. School refusal behaviour: Are children and adolescents with autism spectrum disorder at a higher risk? Research in Autism Spectrum Disorders. 2017;41-42:31-38.